A 75 year old female was brought to casualty with c/o feeling drowsiness
This is an online e log book to discuss our patient de-identified health data shared after taking his/her/guardians singned informed consent. Here we discuss our individual patients problems with an aim to solve the patient’s clinical problem with collective current best evident based input.
This E blog also reflects my patient cantered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of “patient clinical data analysis” to develop my competency in reading and comprehending clinical data including history, clinical findings,investigations and come up with diagnosis and treatment plan.
This is the case of 75 year old female brought to casuality with complaints of feeling drowsiness
CHIEF COMPLAINT:
Giddiness
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic two days ago.she then developed giddiness in the evening( 16/07/2023)
She then developed weakness of both hands and legs
H/o blurred vision
H/o toddy consumption three days ago
H/o difficulty in hearing
PAST HISTORY:
N/K/C/O Hypertension, Diabetes mellitus,Tb, Thyroid disorders,asthma, epilepsy.
H/o cataract surgery for both the eyes 10 years ago
H/o hysterectomy 4 years ago
Daily routine :
-patient used to wakeup at 6.00am
-she used to sweep her house ,wash clothes,cooks food for herself.
-she used to have breakfast (Rice)at 10am
-she used to play pachisi game with her neighbours till 1pm
-At 1pm she used to have her lunch
-Takes rest upto 4pm
-she used to have toddy at 5pm
-she used to have dinner by 8pm
-Goes to bed by 10pm
Family History:
No significant family history.
Personal History:
Mixed diet
Normal appetite
Adequate sleep
Regular bowel movements
No history of smoking and chewing of tobacco
H/o consumption of toddy daily
GENERAL EXAMINATION:
prior consent was taken and patient was examined in a well lit room.
Patient was conscious, coherent, co-operative
Pallor present
No Icterus
No clubbing
No cyanosis
No generalized lymphadenopathy and bipedal edema.







VITALS :
Temperature-98.1F
BP-110/80mmHg
PR- 78bpm
RR-20 cpm
Spo2-97% at room air
GRBS-116 mg/dl
SYSTEMIC EXAMINATION:
RS: Bilateral symmetrical chest movement and air entry
CVS: S1,S2 heard
No murmurs
PA: soft, no tenderness and distension
CNS : NF NB
Sensory and motor system normal
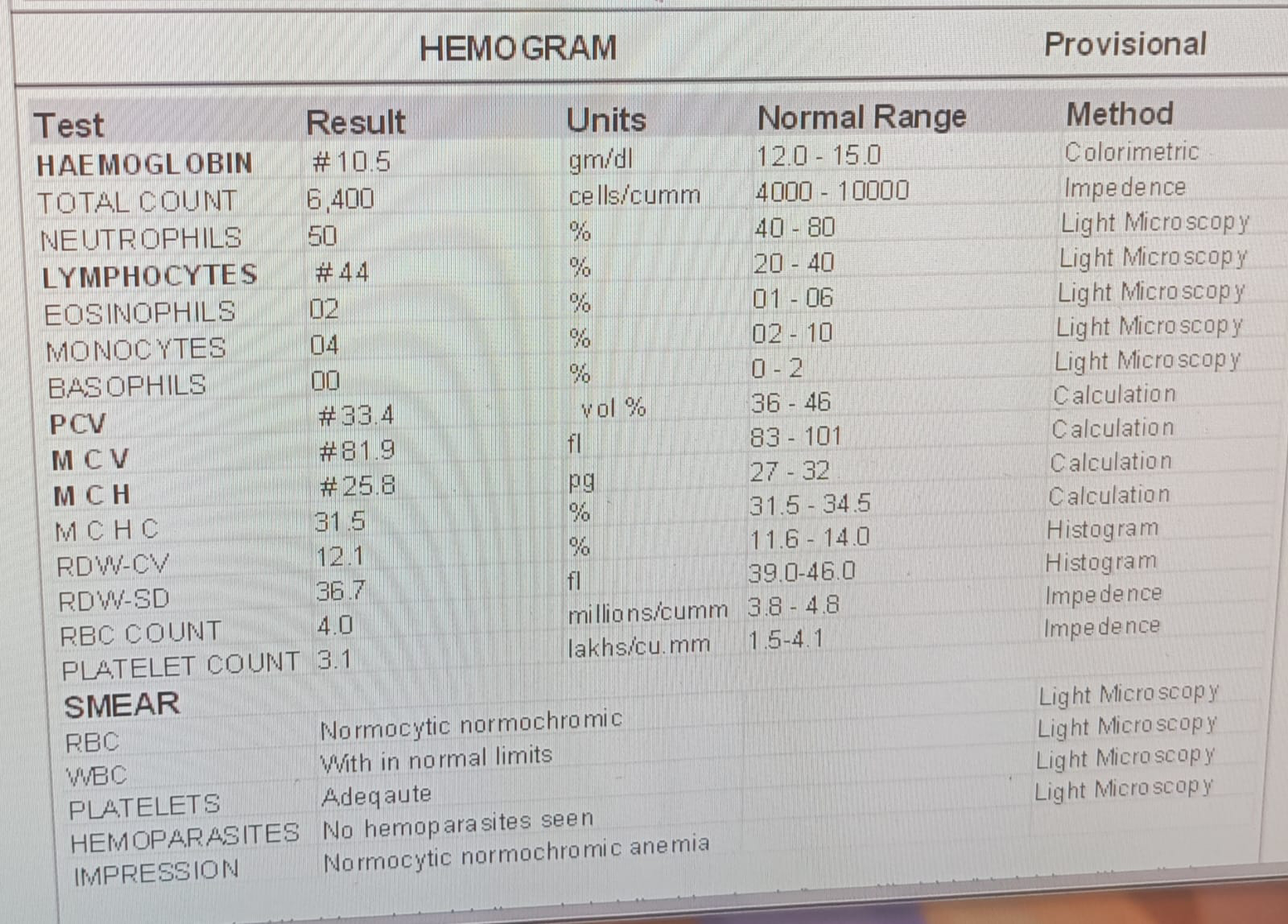
Investigations: